8 Conduction Defects at the AV Node
The AV node is the primary pathway for signals originating in the atria to reach the ventricles. It really has two functions: first is to allow the SA node signal to transit to the ventricle. However, if this transit was immediate, then the atrial and ventricles would contract at the same time rather than sequentially. Therefore, the second role of the AV node is to cause a slight delay in signal transit, allowing the atria to contract first, followed by the ventricles.
There are several measurements one can take with respect to the timing of waves and segments on the ECG. These will be covered in detail in the chapter examining 12 lead ECG interpretation. For now, let’s just focus on the aspects related to the SA node firing and the AV node delay.
The P wave indicates the initiation of the SA node firing, and the QRS complex represents ventricular firing. Between the P wave and the QRS there is a flat segment representing time in the AV node (thus no electrical signal). So, we can measure this SA node firing and AV conduction delay by charting the time from P wave onset to the QRS onset. This is the PR Interval. A normal PR interval duration is between 0.12 and .20s.
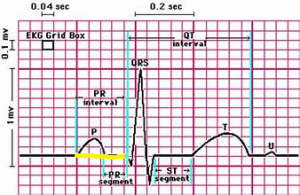
Let’s measure the PR interval on a normal ECG:
Now that we understand what is happening during the PR interval, we can begin to examine defects that may occur in the AV node to disrupt, delay and even block signals from passing through the AV node, causing a loss of ventricular beats. These disruptions are referred to as AV blocks. The degree of severity is classified as first, second, and third-degree AV blocks. Let’s look at each one of these defects.
First degree AV Block
A first-degree AV block is not really a block at all. It is simply a delay at the AV node that is longer than the normal 0.12- 0.20s delay. It may be a normal variant seen in a small percentage of the population or related to increased vagal tone. In any event, we still see a sinus rhythm, so always do the typical assessment of rate and rhythm but add the attribution of first-degree AV block (example “Normal Sinus Rhythm with a first degree AV block”).
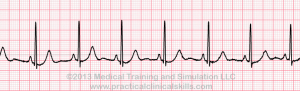
Let’s work an example:

Atrial rate: 80 bpm Ventricular rate: 80 bpm PR interval: .28s. Interpretation: Normal Sinus Rhythm with a First Degree AV Block.
How did you do? Did you take a 3-cycle average to get an average heart rate? For the PR interval, did you count the number of small boxes (7) and then multiply by time per box (0.04)?
Try a more dramatic example. Notice how the P waves are tough to spot. Hiding among the T wave!

Atrial rate : 98 Vent. Rate 98 PR interval ____? Interpretation ________ with__________
The first-degree AV block does not carry any clinical significance and does not affect the ventricular rate. The exercise science professional should make note of the AV block and of course be cognizant of any change in the ECG from the initial assessment.
Second Degree AV Block: Type I and Type II
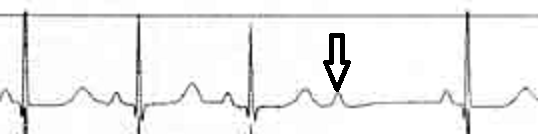
To introduce the second-degree AV block, we need to first understand the term “Dropped Beat”. A dropped beat is when you have a sinus beat (p wave) but it does not get through the AV node, and therefore there is no associated QRS. See the example below:
With the second-degree AV blocks there are dropped beats. However, there are two distinct patterns of how these dropped beats occur, and therefore we have a Type I second degree AV block and a Type II. The key to identifying these types of AV block will be by examining the PR intervals.
Second Degree AV Block- Type I
Often called a Wenckebach block, the second-degree AV block type I has two distinct features:
- Dropped beats are evident
- PR interval progressively lengthens until there is a dropped beat, then the PR interval resets
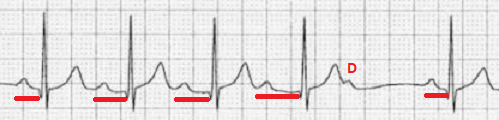
Look at the example below:
Now you try:

Look at the PR intervals in figure 7. Are they the same, or do they progressively lengthen (they do)?
Is there a PR reset after the dropped beat (why yes, there is!)?
Atrial rate: 68bpm (average of first 3). Ventricular rate: Due to dropped beat, use the entire strip (4 cycles): 54bpm
Interpretation: Second Degree AV Block Type I
Why didn’t we say normal sinus rhythm? Well, the dropped beats mean that there is NOT a p wave matched with a QRS for each cycle, so this rhythm has a stand-alone name.
Causes of 2nd degree block? AV blocks may be transient in nature, due to cardiac surgery, or may be due to some type of cardiac injury (myocarditis, infarction) and some medications that affect AV refractory time. The ventricular rate could potentially be so low that the patient becomes hemodynamically unstable (low blood pressure, dizziness). For prolonged or permanent significant AV blocks a pacemaker may be indicated.
Second degree AV Block- type II
First, let’s look at the following ECG:
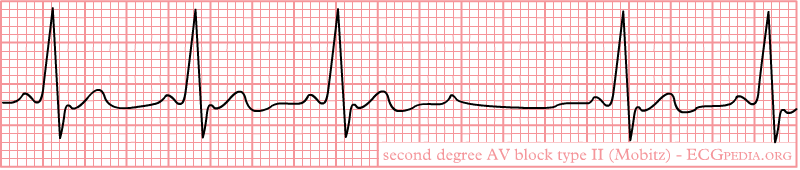
Now look at the PR intervals, are they: The same? or Progressively lengthening?
I’m hoping you will see that in this case the PR intervals are the same. In the second-degree AV block type II we will see:
- Dropped beats, consistent or possibly changing in ratio
- PR intervals are unchanged
If there are several dropped beats, the ventricular rate can be quite low, and the patient may be “hemodynamically compromised” (low cardiac output, low blood pressure).

The second-degree AV block type II is slightly different than type I in the probable location of the defect. It is more likely the defect is in the bundle of His, rather than the AV node. Like Type I, the causes may be due to cardiac injury, medications that increase vagal tone, and cardiac surgery. Type II is more often associated with hemodynamic compromise, and progression to third degree AV block.
Third Degree AV Block: Complete Heart Block
Imagine taking some scissors and cutting the link between the atria and the ventricle completely. All atrial activity (P waves) would be blocked from influencing the ventricles, and the ventricles would have to pace themselves! Since ventricular pacing is very slow, this will no doubt compromise the patient. In the third-degree AV block (also called a complete heart block) there is no SA node pacing communication through the AV node to the ventricles, and the chambers pace themselves. On the ECG you will not see a PR interval pattern, as there is a complete dissociation between the atria and ventricles.
Identifying the third-degree AV block can sometimes be confusing. I suggest that when you see the dropped beats, rule out both of the second-degree blocks:
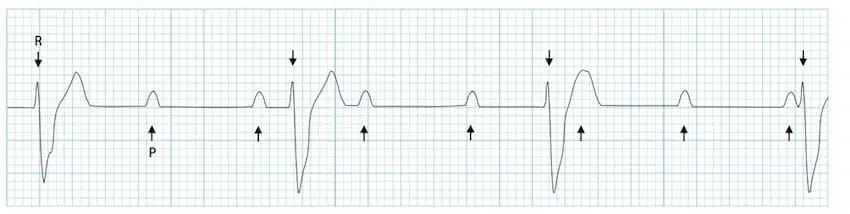
- Do you see the dropped beats?
- Now look at the PR intervals, are they: The same? or Progressively lengthening?… or Neither ?
In this case the PR intervals look like they get longer, then shorter, it makes no sense! It can’t be either of the second-degree av blocks. That should clue you in that you may be looking at a 3rd degree AV block. In this example the atrial rate is about 100bpm, while the wide complex (paced in ventricle) ventricular rate is about 39bpm.
Try another one:

- – Do you see the dropped beats ?
- – Now look at the PR intervals, are they: The same? or Progressively lengthening?.. or Neither ?
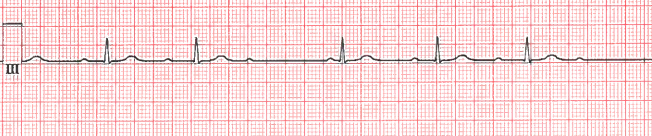
Atrial Rate?______ Ventricular rate? ______ Interpretation : Third Degree AV Block
In this example the P waves are quite small. If you map out their pacing, you may note that some of the P waves are hidden within the ventricular cycle, so this can get challenging!
While the causes of the third-degree AV block may be the same as the second degree, this is a significant rhythm disturbance that can lead to lethal arrhythmias. A pacemaker is usually warranted to connect the atrial firing to the ventricle to restore normal heart pacing.
Mini Quiz! See if you can identify the rhythms (you may have to determine rate)



Answers
Figure 12- Second degree AV block type II
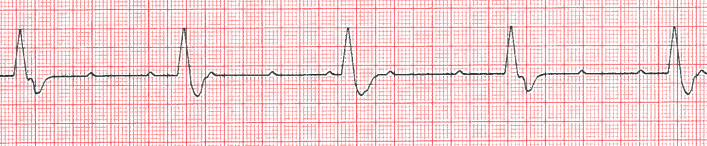
Figure 13- Normal Sinus Rhythm (did I fool you?)
Figure 14- NSR with a first-degree AV block
Figure 15- Third degree AV block
Figure 16- Second degree AV block type I (Wenckebach)
Selected Sources
Goldberger’s Clinical Electrocardiography: A simplified approach 10th ed. Goldberger A., Goldberger, Z, Shvilkin A. Elsevier pub. ISBN-10 0323824757 2023.
Clinical Exercise Electrocardiography – Levine S., Coyne B., Colvin L. Jones & Bartlett Learning Pub. ISBN-10 1284034208 2015.
